最新版 CASP RCT Checklist 中文版教學

教學說明
實證醫學是否時常讓你頭痛?
你是否以為實證醫學就是要學會超複雜的「統計方法」?
事實上,一般醫院要求的實證醫學報告都是希望幫助你了解實證醫學的「基本觀念」,讓你不要盲目的相信研究結果。
這份教學不會有複雜的統計數學,只會有實證醫學的基本觀念,希望可以幫助你快速完成實證醫學報告。
版本比較
2014 年版
- A: 研究結果可信嗎?
- B: 研究結果為何?
- C: 研究結果對於當地病人有幫助嗎?
2020 年版
- A: 隨機對照試驗的基本研究設計是否有效?
- B: 研究方法是否嚴謹?
- C: 結果是什麼?
- D: 結果對於當地是否有幫助?
Word 檔下載連結
CASP-Randomised-Controlled-Trial-Checklist隨機對照試驗檢核表下載
Section A:隨機對照試驗的基本研究設計是否有效?
Is the basic study design valid for a randomised controlled trial?
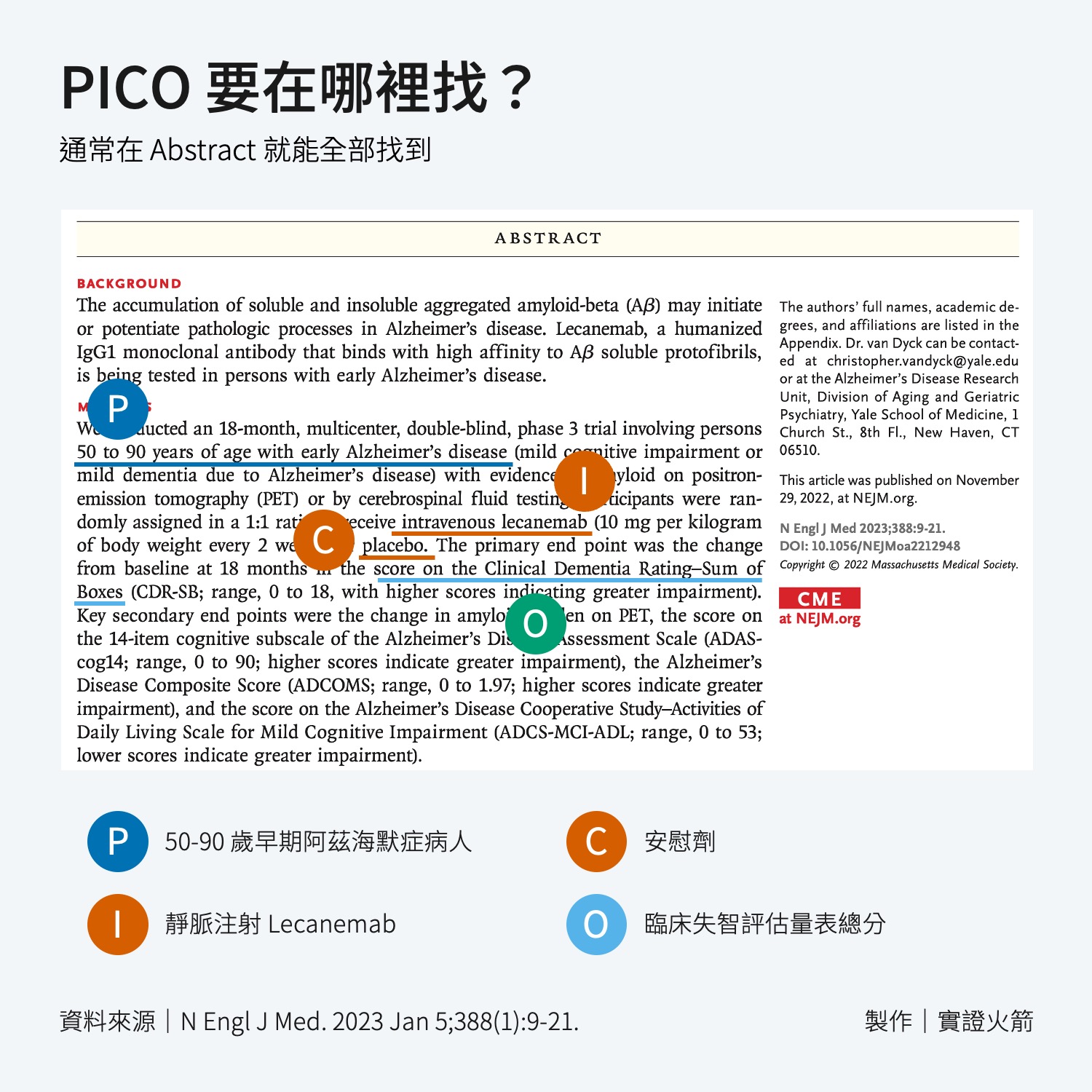
問題 1:這項研究是否聚焦於一個清楚的問題?
Did the study address a clearly focused research question?
原文提示
- Was the study designed to assess the outcomes of an intervention?
此研究是否設計來評估一種介入的結果? - Is the research question ‘focused’ in terms of:
- 研究族群Population studied
- 介入措施Intervention given
- 對照組的選擇Comparator chosen
- 結果測量Outcomes measured
教學
與你設定的 PICO 是否符合?
問題 2:受試者是否被隨機分派到不同組別?
Was the assignment of participants to interventions randomised?
原文提示
- How was randomisation carried out? Was the method appropriate?
隨機分配方式為何?該方法是否合適? - Was randomisation sufficient to eliminate systematic bias?
隨機分配方式是否足以消除系統性偏差? - Was the allocation sequence concealed from investigators and participants?
分配序號是否對實驗者與受試者隱藏?
教學
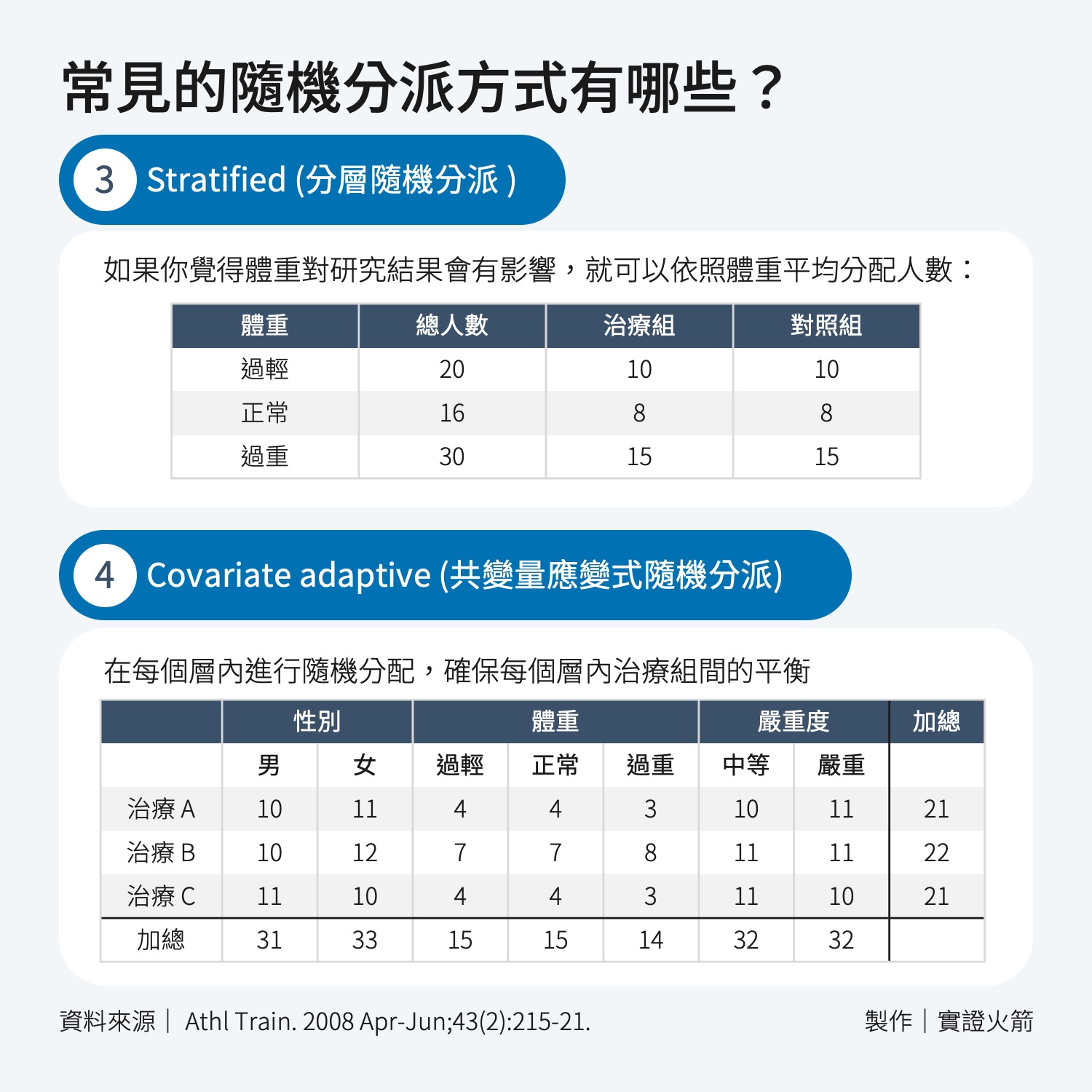
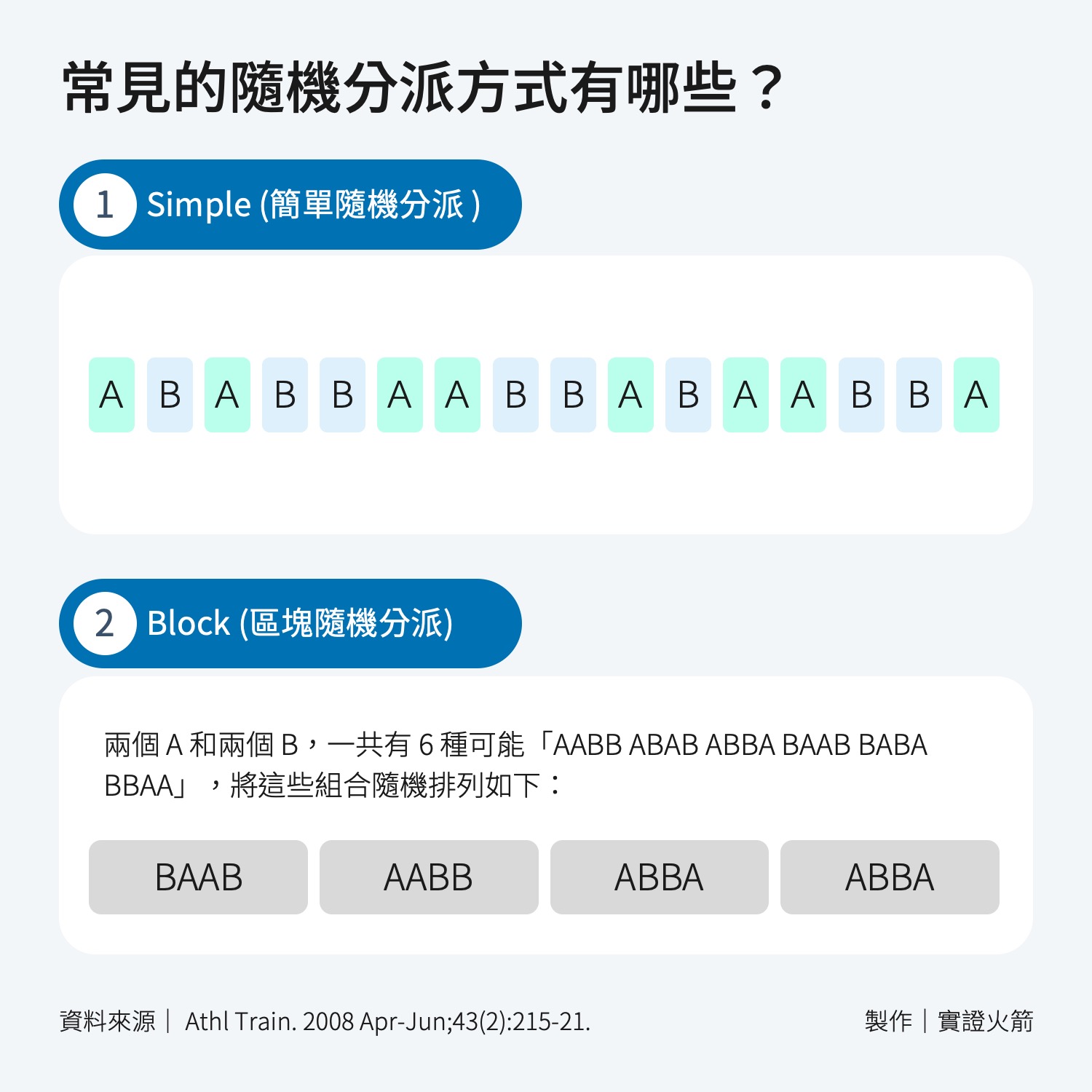
通常在「Method」可以找到,常見的隨機分派方式1包含:
- Simple:人數大於 200 人時可以使用
- Block:人數較少時,就要用 Block
- Stratified:某些特質會影響研究結果時使用。
- Covariate adaptive:會影響研究的特徵(Baseline Characteristics)非常多時使用,在每個層內進行隨機分配,確保在各層內的治療組間基線特徵得到平衡。
- Minimization method:也用於平衡多種基本特徵,但其特點在於針對「每一個新加入的受試者」進行即時計算,確定將其分配到哪個組能使基線特徵的不平衡最小化。
問題 3:是否所有進入試驗的受試者在研究結論當中均被適當的考量過?
Were all participants who entered the study accounted for at its conclusion?
原文提示
- Were losses to follow-up and exclusions after randomisation accounted for?
是否納入隨機分配後失去追蹤與排除的患者? - Were participants analysed in the study groups to which they were randomised (intention-to-treat analysis)?
受試者是否按照他們被隨機分配的研究進行分析(治療意向分析法)? - Was the study stopped early? If so, what was the reason?
試驗是否提早終止?若有,原因為何?
教學
在檔案中搜尋有無以下三個詞:Intention-to-treat, As treated, Per-protocol
- Intention-to-treat(意象分析):所有隨機分配受試者均分析。
- As treated(實際治療分析):按實際接受的治療分析。
- Per-protocol(符合計畫書分析):僅分析完全遵守試驗計畫(Protocol)者。
可以分析的人數分別為 1>2>3
以這篇 NEJM 的案例來看:
- 一共有 233 人分到安慰劑組,最後符合計畫書(Protocol)完成治療的有 201 人。
- 一共有 235 人分到 60 毫克組,最後符合計畫書(Protocol)完成治療的有 204 人。
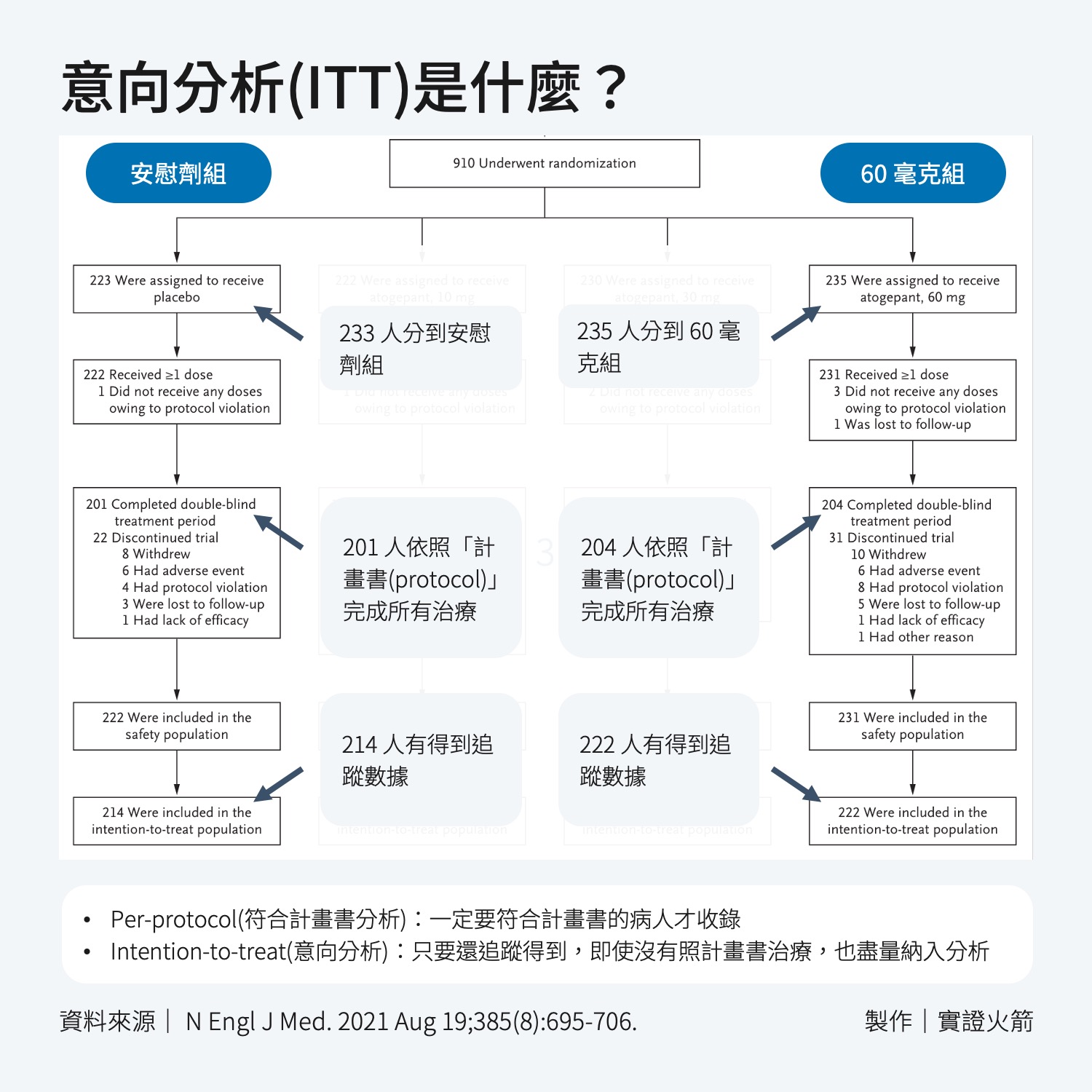
如果只分析符合計畫書的 201 和 204 人,就叫做 Per-protocol;如果把停止治療,但還能追蹤到數據的病人都納入,也就是 214 人和 222 人,就叫做 Intention-to-treat。
常見問題:為什麼需要 Intention-to-treat 呢?
你可以想像一個情境:如果其中一組病人因為「症狀急遽加重」而大量退出試驗。在這樣的情況下,如果只分析剩下的病人,就會有很大的「偏誤」(Bias)。
Section B:研究的方法是否嚴謹?
Was the study methodologically sound?
問題 4:受試者、健康相關工作人員及研究人員是否盲化?
原文提示
- Were the participants ‘blind’ to intervention they were given?
受試者是否盲化? - Were the investigators ‘blind’ to the intervention they were giving to participants?
研究者(給予介入者)是否盲化? - Were the people assessing/analysing outcome/s ‘blinded’?
研究者(評估/分析結果者)是否盲化?
教學
在研究中,可以被盲化的人包含:
- 病人
- 臨床醫師或照護者
- 數據搜集者
- 檢驗結果判讀者
- 數據分析者
通常 single blind 是指「(1)受試者」;double blind 是指「(1)受試者 + (2)照護者」;triple blind 是指「(1)受試者 + (2)照護者 + (3)(4)(5)分析者」
搜尋「blind」通常就能找到答案,可以在報告中回答研究中有做到以上哪些人的盲化?
問題 5:各組研究對象在一開始進入試驗時的基本特性是否相似?
Were the study groups similar at the start of the randomised controlled trial?
原文提示
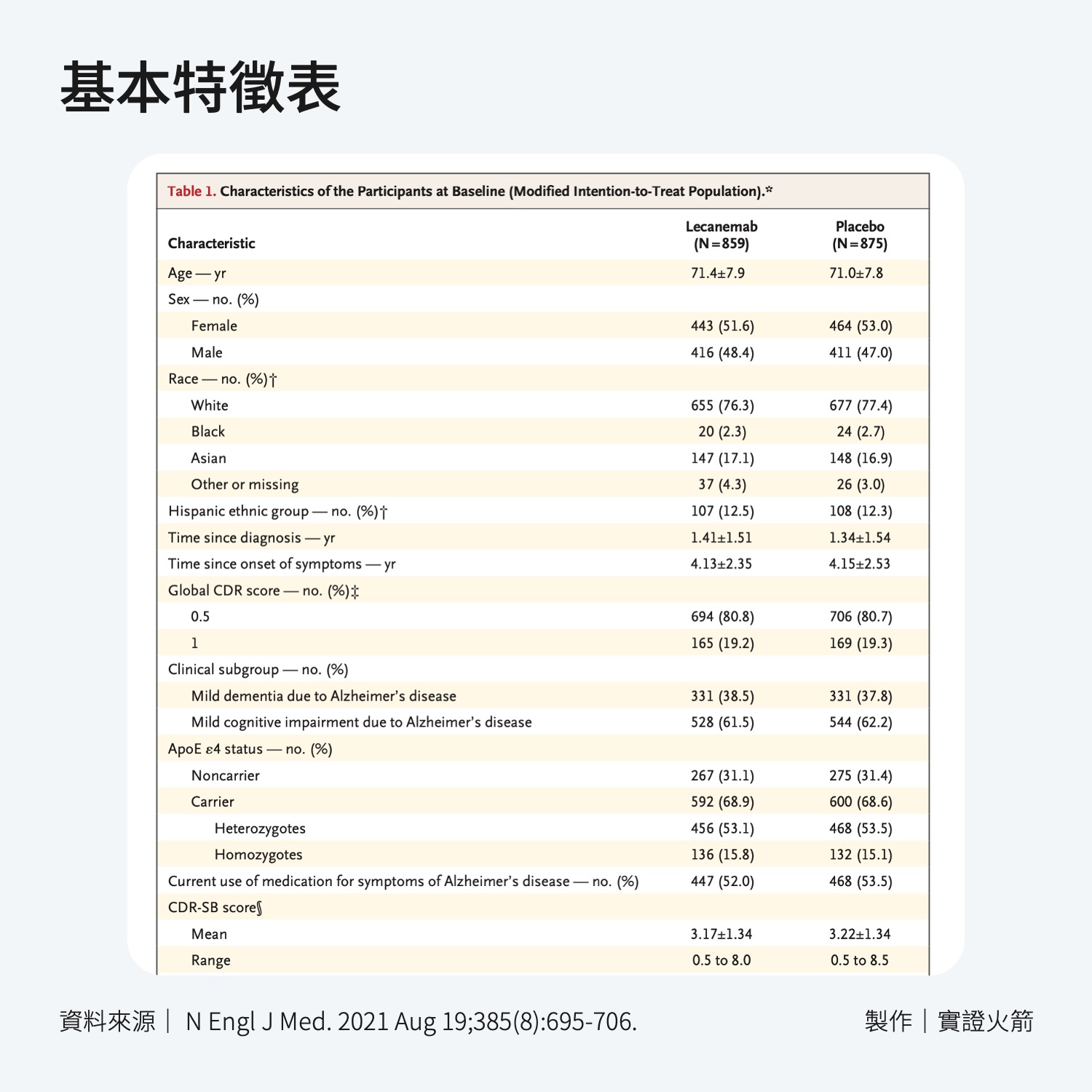
- Were the baseline characteristics of each study group (e.g. age, sex, socio-economic group) clearly set out?
文章中是否清楚呈現各組的基本特徵(如:年齡、性別、社經地位)? - Were there any differences between the study groups that could affect the outcome/s?
組問是否存在可能影響結果的差別?
教學
通常是在 Table 1.,如果有附上 P 值,可以檢查是否都有大於 0.05 ,表示兩組間沒有顯著差異。
進階一點的評讀方式,應該思考文章有沒有少列入哪些可能影響結果的基本特性,常見影響研究的特性包含:
- 性別
- 年齡
- 種族
- 疾病嚴重度
- 共病症
- 過去與現在接受過的治療
- 社會經濟地位
問題 6:除了實驗的介入措施之外,各組的所有對待是否相同?
Apart from the experimental intervention, did each study group receive the same level of care (that is, were they treated equally)?
原文提示
- Was there a clearly defined study protocol?
試驗計畫是否清楚定義? - If any additional interventions were given (e.g. tests or treatments), were they similar between the study groups?
若有給予額外介入(檢查或治療),各組給予的介入是否相似? - Were the follow-up intervals the same for each study group?
各組的追蹤期是否相同?
教學
通常在「Method」可以找到答案。
Section C:結果是什麼?
What are the results?
問題 7:介入措施的效果是否有被完整報告?
Were the effects of intervention reported comprehensively?
原文提示
- Was a power calculation undertaken?
是否有計算檢定力? - What outcomes were measured, and were they clearly specified?
研究中測量哪些結果?是否明確定義? - How were the results expressed? For binary outcomes, were relative and absolute effects reported?
結果是如何表達的?對於二元結果,是否報告了相對和絕對效應? - Were the results reported for each outcome in each study group at each follow-up interval?
是否列出每一組在每次追蹤時的數據? - Was there any missing or incomplete data?
是否有遺漏或是不完整的資料? - Was there differential drop-out between the study groups that could affect the results?
不同組間的退出率是否足以影響結果? - Were potential sources of bias identified?
是否列出潛在的偏差來源? - Which statistical tests were used?
使用到哪些統計方法? - Were p values reported?
是否列出p值?
教學
- 檢定力(Power):研究之前,通常會計算需要收入多少個案才能比較出治療效果的差異(或證明沒有差異)。
- 測量結果:可以上網查該疾病的常用量表,或是研究中的量表是否是公認的指標。
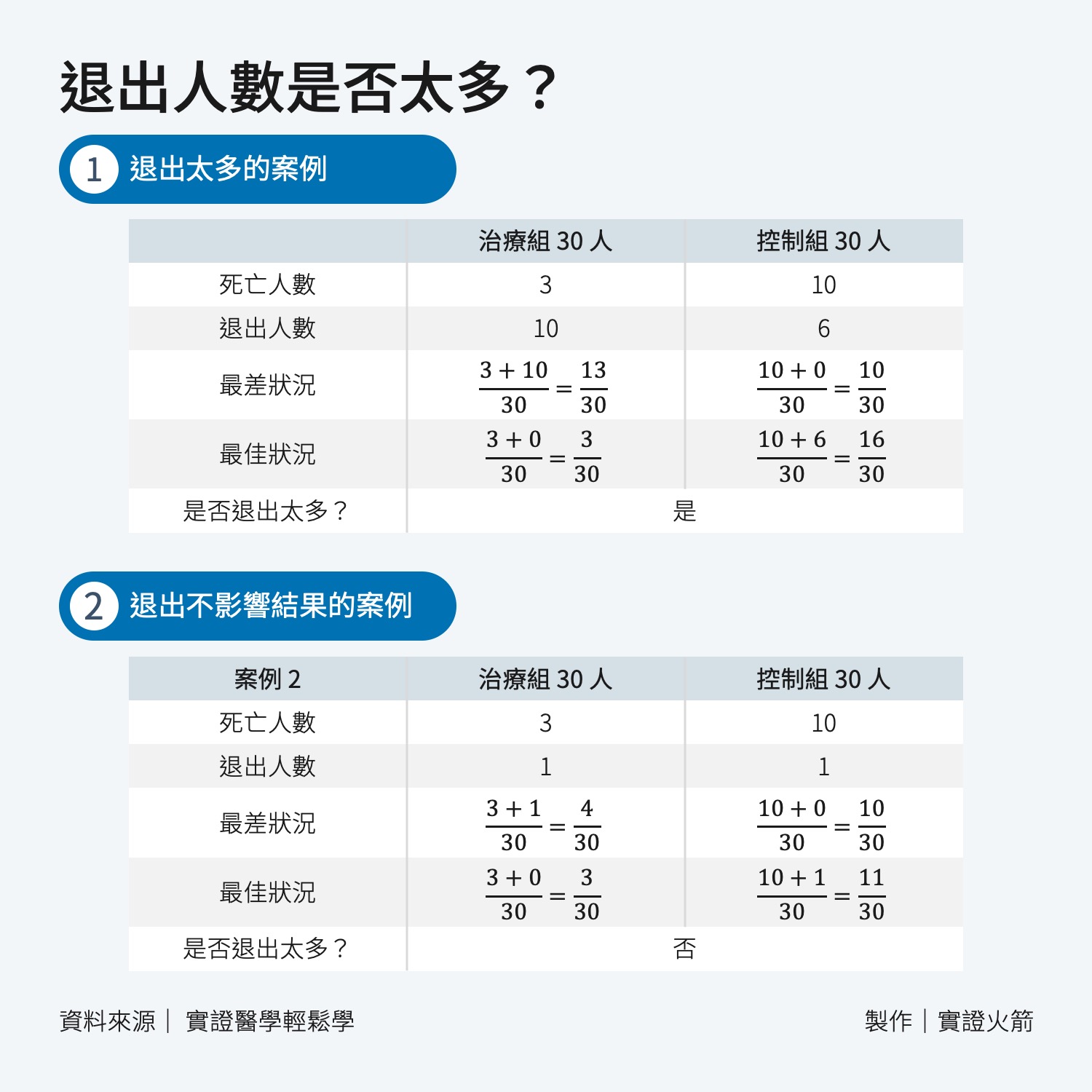
- 退出率:研究中的「Discussion」中通常會提到,有些研究會透過「敏感度測試」來驗證,舉例如下:
「The dropout rate was 17.2%, and a sensitivity analysis that evaluated the effect of missed doses was consistent with the primary end-point analysis」
你也可以自己計算退出人數是否太多,如下圖教學:
常見評估效果的指標有:
Odds Ratio (勝算比)
兩組事件發生與不發生的比值比。
舉例:「抽菸有肺癌/抽菸無肺癌」除以「無抽菸有肺癌/無抽菸無肺癌」
Relative Risk (相對風險)
舉例:吃 A 藥能讓疾病風險從 5% 下降到 0.5%,兩者相除等於 10 倍。
Absolute Risk Reduction (絕對風險減少)
舉例:吃 A 藥能讓疾病風險從 5% 下降到 0.5%,兩者相減等於下降 4.5%。
Relative Risk Reduction (相對風險減少)
舉例:吃 A 藥能讓疾病風險從 5% 下降到 0.5%,兩者減去了 90% 的風險(從 5% 變成 0.5%)。
Hazard Ratio (風險比)
舉例:
- 在治療組中,有30%的患者在觀察期內去世。
- 在對照組中,有50%的患者在觀察期內去世。
這個風險比0.6表示,相較於對照組,治療組的患者在觀察期內死亡的速率是對照組的60%。換句話說,新藥治療使得患者死亡的風險降低了40%。
Median Survival Time Difference (中位生存時間差異)
舉例:
- 對照組:中位生存時間為12個月。
- 治療組:中位生存時間為18個月。
中位生存時間差異=18個月−12個月=6個月
Cohen’s d
說明:兩組均數差異的標準化效應量。聽不懂沒關係,因為牽扯到複雜的數學公式,可以知道結果就好。
- 0.2 表示小效應
- 0.5 表示中等效應
- 0.8 或以上表示大效應
Hedges’ g
Cohen’s d 的修正版本,適用於小樣本。
問題 8:是否有列出介入/治療的精確度?
Was the precision of the estimate of the intervention or treatment effect reported?
原文提示
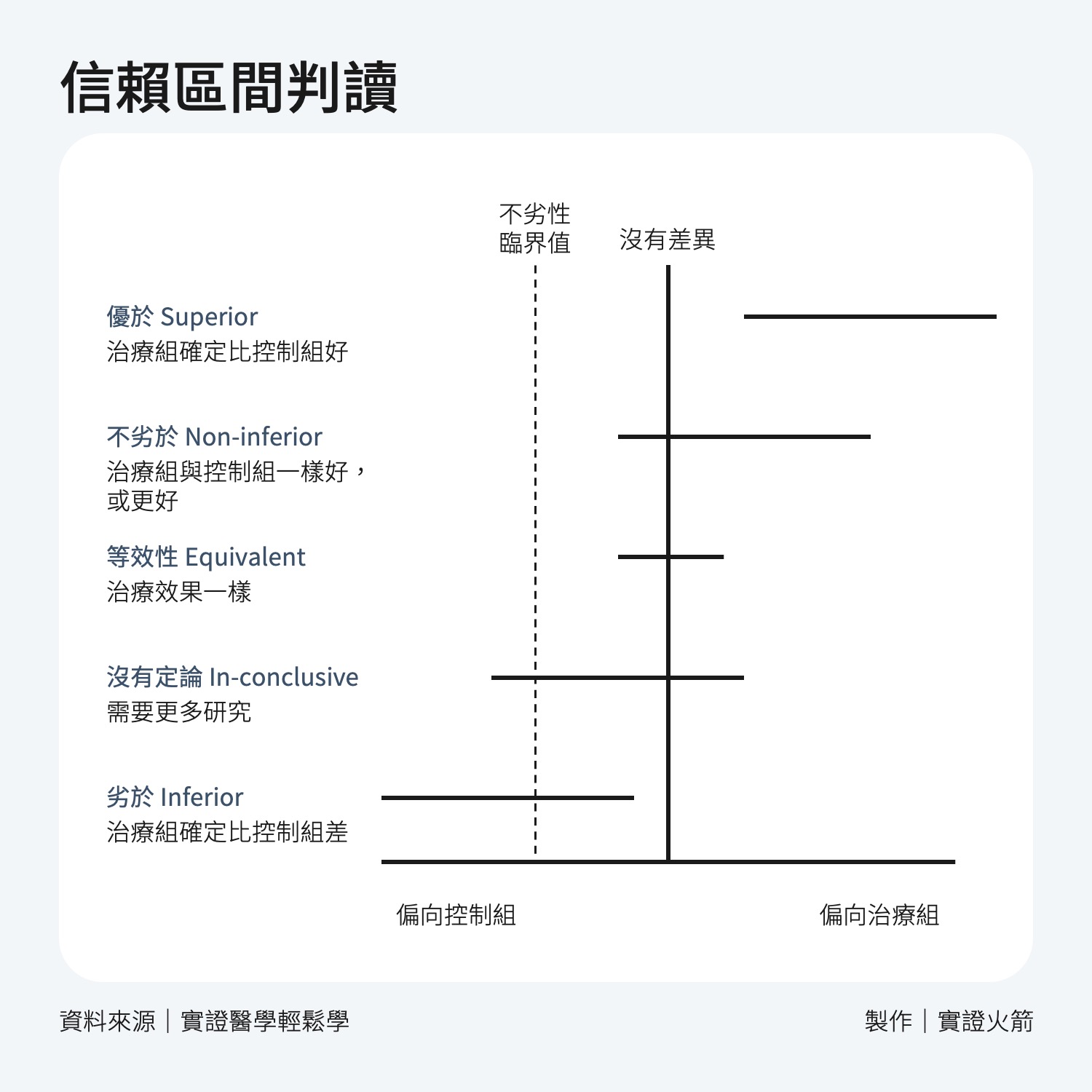
- Were confidence intervals (CIs) reported?
是否列出信賴區間?
教學
假設一項新藥物的臨床試驗結果如下:
- 治療組平均降低血壓5 mmHg
- 95%信賴區間為[1 mmHg, 9 mmHg]
這表示我們有 95% 的信心,真實的治療效果會落在 1 到 9 mmHg之間,雖然沒有跨過 0 mmHg,表示這款新藥是有效果的。
但實際效果可能從幾乎無效(1 mmHg)到非常顯著(9 mmHg),導致結果不確定,因此我們會認為信賴區間過大。
問題 9:介入措施所帶來的效益是否值得付出傷害及成本的代價?
Do the benefits of the experimental intervention outweigh the harms and costs?
原文提示
- What was the size of the intervention or treatment effect?
介人或治療的效果有多好(大)? - Were harms or unintended effects reported for each study group?
是否列出各組中發生的不良效應? - Was a cost-effectiveness analysis undertaken? (Cost-effectiveness analysis allows a comparison to be made between different interventions used in the care of the same condition or problem.)
是否進行成本效益評估(成本效益分析能比較用於同一病症或問題中的不同介入措施)?
教學
搜尋「adverse effect」,通常可以找到一個完整的表格
Section D:結果對於當地是否有幫助?
Will the results help locally?
以下的教學會放在 Apply
問題 10:研究結果是否可以應用在你的情境當中(或當地族群?)?
Can the results be applied to your local population/in your context?
原文提示
- Are the study participants similar to the people in your care?
受試族群是否與您照顧的患者相似? - Would any differences between your population and the study participants alter the outcomes reported in the study?
你的患者(們)與本研究受試者群組的差異是否會影響到研究得出的結果? - Are the outcomes important to your population?
研究結果對你的族群是否重要? - Are there any outcomes you would have wanted information on that have not been studied or reported?
是否有您想要的結果或資訊尚未被研究或提出? - Are there any limitations of the study that would affect your decision?
本研究是否有任何限制會影響到您的決策?
問題 11:研究中的介入方法對您的患者們是否比起任何現存介入方式更有價值?
原文提示
Would the experimental intervention provide greater value to the people in your care than any of the existing interventions?
- What resources are needed to introduce this intervention taking into account time, finances, and skills development or training needs?
本介入方式所需要的時間、費用、技術訓練成本為何? - Are you able to disinvest resources in one or more existing interventions in order to be able to re-invest in the new intervention?
您是否可以將投入在現有介入方式的資源挪動至新的介入方式上?
參考資料
-
Kang M, Ragan BG, Park JH. Issues in outcomes research: an overview of randomization techniques for clinical trials. J Athl Train. 2008 Apr-Jun;43(2):215-21. doi: 10.4085/1062-6050-43.2.215. PMID: 18345348; PMCID: PMC2267325. ↩